Further Information, Publications,...
Transarterial Chemoperfusion (TACP)
Dear Patients,
In the following pages we would like to inform you about the Transarterial Chemoperfusion (TACP).
The procedure of TACP is based on the principle of selective regional application of chemotherapeutic substance. The concentration of cytostatic drug within the tumor defines the extent of destruction of the tumor cells.
Procedure of the treatment
The patient is informed about the procedure and the risks and adverse reactions associated with the arterial intervention and cytostatis drug application and consent obtained. Inorder to reduce acute symptoms like epigastric pain or nausea during the TACP an infusion with Opioid and if required some glucocorticoid is connect intravenously. After disinfection and local anaesthesia the femoral artery is punctured with Seldinger technique and usually 4F femoral sheath is inserted. The catheterization is mostly done
using the Pigtail, Renegade, Cobra, Sidewinder and Headhunter catheters. After an orientation upper abdomen angiography, a catheter is selectively placed in the coeliac trunk through which chemoperfusion of a large part of tumor tissue can be achieved. In our institute we use coaxial tracker catheter for super selective catheterisation of tumor supplying artery. After the correct catheter placement chemotherapeutic agents Mitomycin C and Gemcitabine are infused for about an hour using a perfusion pump at a dose of 8,5 mg/m2 and 1000 mg/m2 respectively. After completion of perfusion therapy the catheters and femoral sheath are removed and the puncture site draped in a pressure bandage for about 6 hours during which he or she is observed for possible complications. A complete TACP-therapy consists angiography guided chemoperfusion, MRI follow-up on the same day and a CT follow-up the following day without contrast media 24 to 48 hours after the therapy. Typically TACP is performed 2 to 3 times with a gap of 4 weeks between the therapies.
Therapy success

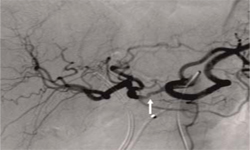
A 56-years-old patient with diffuse infiltrating pancreas carcinoma in hilum of liver. The liver showed 3 small nodular metastases (not seen here, in follow-up with complete remission).

The same findings after seven sittings of TACP. The tumor infiltrated region is now seen as a homogenous region and radiologically there is no evidence of a tumor.

9 months after the TACP no evidence of tumor - a complete response.